Posterior Tibial Tendon Dysfunction Physical Therapy
Overview
The adult acquired flatfoot (AAF) is a progressive, symptomatic (painful) deformity resulting from gradual stretch (attenuation) of the tibialis posterior tendon as well as the ligaments that support the arch of the foot. Although the posterior tibialis tendon plays a significant role, this pathology has recently been recognized as involving failure of other interosseous ligaments, such as the spring ligament. Due to the complexity of this pathology, posterior tibial tendon dysfunction (PTTD) is now referred to as adult acquired flatfoot. Severe flatfoot associated with AAF can lead to other problems, such as plantar fascial tension, tendon pain, rearfoot subluxation, and ankle osteoarthritis. 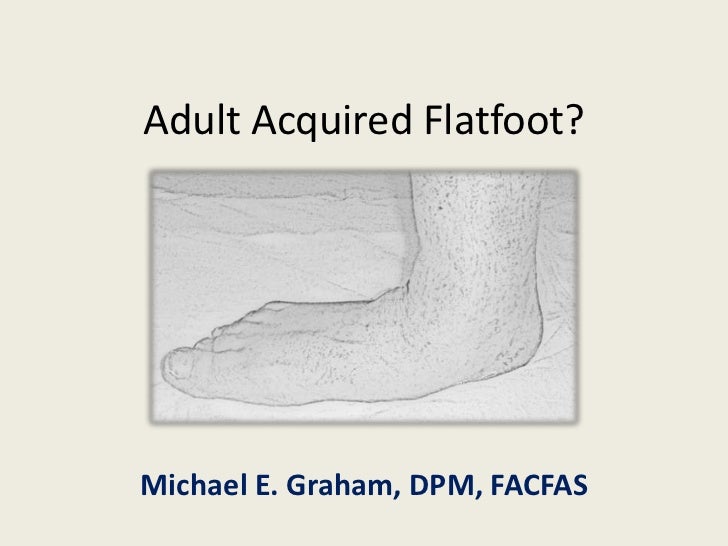
Causes
Adult flatfoot typically occurs very gradually. If often develops in an obese person who already has somewhat flat feet. As the person ages, the tendons and ligaments that support the foot begin to lose their strength and elasticity.
Symptoms
The types of symptoms that may indicate Adult-Acquired Flat Foot Deformity include foot pain that worsens over time, loss of the arch, abnormal shoe wear (excessive wearing on the inner side of shoe from walking on the inner side of the foot) and an awkward appearance of the foot and ankle (when viewed from behind, heel and toes appear to go out to the side). It is important that we help individuals recognize the early symptoms of this condition, as there are many treatment options, depending upon the severity, the age of the patient, and the desired activity levels.
Diagnosis
The diagnosis of tibialis posterior dysfunction is essentially clinical. However, plain radiographs of the foot and ankle are useful for assessing the degree of deformity and to confirm the presence or absence of degenerative changes in the subtalar and ankle articulations. The radiographs are also useful to exclude other causes of an acquired flatfoot deformity. The most useful radiographs are bilateral anteroposterior and lateral radiographs of the foot and a mortise (true anteroposterior) view of the ankle. All radiographs should be done with the patient standing. In most cases we see no role for magnetic resonance imaging or ultrasonography, as the diagnosis can be made clinically.
Non surgical Treatment
What are the treatment options? In early stages an orthotic that caters for a medially deviated subtalar joint ac-cess. Examples of these are the RX skive, Medafeet MOSI device. Customised de-vices with a Kirby skive or MOSI adaptation will provide greater control than a prefabricated device. If the condition develops further a UCBL orthotic or an AFO (ankle foot orthotic) could be necessary for greater control. Various different forms of surgery are available depending upon the root cause of the issue and severity. 
Surgical Treatment
If surgery is necessary, a number of different procedures may be considered. The specifics of the planned surgery depend upon the stage of the disorder and the patient?s specific goals. Procedures may include ligament and muscle lengthening, removal of the inflamed tendon lining, tendon transfers, cutting and realigning bones, placement of implants to realign the foot and joint fusions. In general, early stage disease may be treated with tendon and ligament (soft-tissue) procedures with the addition of osteotomies to realign the foot. Later stage disease with either a rigidly fixed deformity or with arthritis is often treated with fusion procedures. If you are considering surgery, your doctor will speak with about the specifics of the planned procedure.