Pes Planus Causes And Treatment
Overview

If you look at an adult foot from the inside, you'll usually notice an upward curve in the middle. This is called an arch. Tendons, tight bands that attach at the heel and foot bones form the arch. Several tendons in your foot and lower leg work together to form the arches in your foot. When the tendons all pull the proper amount, then your foot forms a moderate, normal arch. When tendons do not pull together properly, there is little or no arch. This is called flat foot or fallen arch.
Causes
Flat feet are a common condition. In infants and toddlers, the arch is not developed and flat feet are normal. The arch develops in childhood. By adulthood, most people have developed normal arches. When flat feet persist, most are considered variations of normal. Most feet are flexible and an arch appears when the person stands on his or her toes. Stiff, inflexible, or painful flat feet may be associated with other conditions and require attention. Painful flat feet in children may be caused by a condition called tarsal coalition. In tarsal coalition, two or more of the bones in the foot fuse together. This limits motion and often leads to a flat foot. Most flat feet do not cause pain or other problems. Flat feet may be associated with pronation, in which the ankle bones lean inward toward the center line. When the shoes of children who pronate are placed side by side, they will lean toward each other (after they have been worn long enough for the foot position to remodel their sole). Foot pain, ankle pain, or lower leg pain (especially in children) may be a result of flat feet and should be evaluated by a health care provider. Adults can develop a flat foot when they are 60 - 70 years old. This type of flat foot is usually on one side.
Symptoms
The primary symptom of fallen arches is painful or achy feet in the area in which the foot arches or on the heel. This area may become swollen and painful to stand still on. This causes the patient to improperly balance on their feet which in turn will cause other biomechanical injuries such as back, leg and knee pain.
Diagnosis
Your doctor examines your feet to determine two things, whether you have flat feet and the cause or causes. An exam may include the following steps, Checking your health history for evidence of illnesses or injuries that could be linked to flat feet or fallen arches, Looking at the soles of your shoes for unusual wear patterns, Observing the feet and legs as you stand and do simple movements, such as raising up on your toes, Testing the strength of muscles and tendons, including other tendons in the feet and legs, such as the Achilles tendon or the posterior tibial tendon, Taking X-rays or an MRI of your feet.
What is PES Planovalgus deformity?
Non Surgical Treatment
What we want to do is support the arch and maintain it in that curved position. So what you want is to bring the foot into a position where you hold and support the arch so you can get that correct heel-midfoot-big toe contact. You would achieve that with a level of arch support. People will take different levels of support, if you?re somebody who has movement in your arch, a strong level of support will hold and maintain you whereas if you?re someone whose arch has collapsed it could need more support and a level of correction built into the support to realign you. If you think of it, when your arch drops, it affects your foot but it also has a biomechanical effect on the rest of the body. But nothing that can?t be solved.
Surgical Treatment
This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer).
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
If you look at an adult foot from the inside, you'll usually notice an upward curve in the middle. This is called an arch. Tendons, tight bands that attach at the heel and foot bones form the arch. Several tendons in your foot and lower leg work together to form the arches in your foot. When the tendons all pull the proper amount, then your foot forms a moderate, normal arch. When tendons do not pull together properly, there is little or no arch. This is called flat foot or fallen arch.
Causes
Flat feet are a common condition. In infants and toddlers, the arch is not developed and flat feet are normal. The arch develops in childhood. By adulthood, most people have developed normal arches. When flat feet persist, most are considered variations of normal. Most feet are flexible and an arch appears when the person stands on his or her toes. Stiff, inflexible, or painful flat feet may be associated with other conditions and require attention. Painful flat feet in children may be caused by a condition called tarsal coalition. In tarsal coalition, two or more of the bones in the foot fuse together. This limits motion and often leads to a flat foot. Most flat feet do not cause pain or other problems. Flat feet may be associated with pronation, in which the ankle bones lean inward toward the center line. When the shoes of children who pronate are placed side by side, they will lean toward each other (after they have been worn long enough for the foot position to remodel their sole). Foot pain, ankle pain, or lower leg pain (especially in children) may be a result of flat feet and should be evaluated by a health care provider. Adults can develop a flat foot when they are 60 - 70 years old. This type of flat foot is usually on one side.
Symptoms
The primary symptom of fallen arches is painful or achy feet in the area in which the foot arches or on the heel. This area may become swollen and painful to stand still on. This causes the patient to improperly balance on their feet which in turn will cause other biomechanical injuries such as back, leg and knee pain.
Diagnosis
Your doctor examines your feet to determine two things, whether you have flat feet and the cause or causes. An exam may include the following steps, Checking your health history for evidence of illnesses or injuries that could be linked to flat feet or fallen arches, Looking at the soles of your shoes for unusual wear patterns, Observing the feet and legs as you stand and do simple movements, such as raising up on your toes, Testing the strength of muscles and tendons, including other tendons in the feet and legs, such as the Achilles tendon or the posterior tibial tendon, Taking X-rays or an MRI of your feet.
What is PES Planovalgus deformity?
Non Surgical Treatment
What we want to do is support the arch and maintain it in that curved position. So what you want is to bring the foot into a position where you hold and support the arch so you can get that correct heel-midfoot-big toe contact. You would achieve that with a level of arch support. People will take different levels of support, if you?re somebody who has movement in your arch, a strong level of support will hold and maintain you whereas if you?re someone whose arch has collapsed it could need more support and a level of correction built into the support to realign you. If you think of it, when your arch drops, it affects your foot but it also has a biomechanical effect on the rest of the body. But nothing that can?t be solved.
Surgical Treatment
This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer).
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Understand Heel Pain
Overview

Heel pain is one of the most common conditions treated by podiatrists. It is often a message that something is in need of medical attention. Pain that occurs right after an injury or early in an illness may play a protective role, often warning us about the damage we have suffered. Heel pain is a problem which affects people of all ages and vocations, whether they are active or not and it comes in many different forms. Heel pain can also occur in children usually between the ages of 8 and 13, as they become increasingly active in sporting activities and during the growing phase.
Causes
The most common cause of heel pain in adults is plantar fasciitis, which is an inflammation of the band of tissue in the sole that connects the heel to the toes and forms the natural foot arch. Plantar fasciitis may or may not be complicated by a calcaneal spur, a small bone growth that protrudes out of the heel. Plantar fasciitis may also be referred to as plantar fasciosis. In contrast to fasciitis, which essentially means inflammation, fasciosis refers to degeneration of the tissue. In fact, if left untreated, acute plantar fasciitis may develop into a chronic painful condition, which results in slow and irreversible degeneration of the fascia, hence plantar fasciosis. The location of the pain is usually exactly under the heel but may also occur in the arch of the foot. Pain typical to plantar fasciitis is that which feels worse when arising on to your feet such as in mornings or after sitting down for a while, and usually progresses in severity when left untreated.
Symptoms
The symptoms of plantar fasciitis are pain on the bottom of the heel, pain in the arch of the foot, pain that is usually worse upon arising, pain that increases over a period of months. People with plantar fasciitis often describe the pain as worse when they get up in the morning or after they?ve been sitting for long periods of time. After a few minutes of walking the pain decreases, because walking stretches the fascia. For some people the pain subsides but returns after spending long periods of time on their feet.
Diagnosis
The diagnosis of plantar fasciitis is generally made during the history and physical examination. There are several conditions that can cause heel pain, and plantar fasciitis must be distinguished from these conditions. Pain can be referred to the heel and foot from other areas of the body such as the low back, hip, knee, and/or ankle. Special tests to challenge these areas are performed to help confirm the problem is truly coming from the plantar fascia. An X-ray may be ordered to rule out a stress fracture of the heel bone and to see if a bone spur is present that is large enough to cause problems. Other helpful imaging studies include bone scans, MRI, and ultrasound. Ultrasonographic exam may be favored as it is quick, less expensive, and does not expose you to radiation. Laboratory investigation may be necessary in some cases to rule out a systemic illness causing the heel pain, such as rheumatoid arthritis, Reiter's syndrome, or ankylosing spondylitis. These are diseases that affect the entire body but may show up at first as pain in the heel.
Non Surgical Treatment
Clinical trials are underway investigating the use of radiofrequency to treat plantar fasciitis. It is a simple, noninvasive form of treatment. It allows for rapid recovery and pain relief within seven to 10 days. The radio waves promote angiogenesis (formation of new blood vessels) in the area. Once again, increasing blood flow to the damaged tissue encourages a healing response. Antiinflammatory medications are sometimes used to decrease the inflammation in the fascia and reduce your pain. Studies show that just as many people get better with antiinflammatories as those who don't have any improvement. Since these medications are rarely used alone, it's difficult to judge their true effectiveness. A cortisone injection into the area of the fascia may be used but has not been proven effective. Studies show better results when ultrasound is used to improve the accuracy of needle placement. Cortisone should be used sparingly since it may cause rupture of the plantar fascia and fat pad degeneration and atrophy, making the problem worse. Botulinum toxin A otherwise known as BOTOX has been used to treat plantar fasciitis. The chemical is injected into the area and causes paralysis of the muscles. BOTOX has direct analgesic (pain relieving) and antiinflammatory effects. In studies so far, there haven't been any side effects of this treatment.
Surgical Treatment
If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints or a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as open surgery, where the section of the plantar fascia is released by making a cut into your heel or endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team.
how to get rid of heel spurs
Prevention

Being overweight can place excess pressure and strain on your feet, particularly on your heels. Losing weight, and maintaining a healthy weight by combining regular exercise with a healthy, balanced diet, can be beneficial for your feet. Wearing appropriate footwear is also important. Ideally, you should wear shoes with a low to moderate heel that supports and cushions your arches and heels. Avoid wearing shoes with no heels.
Heel pain is one of the most common conditions treated by podiatrists. It is often a message that something is in need of medical attention. Pain that occurs right after an injury or early in an illness may play a protective role, often warning us about the damage we have suffered. Heel pain is a problem which affects people of all ages and vocations, whether they are active or not and it comes in many different forms. Heel pain can also occur in children usually between the ages of 8 and 13, as they become increasingly active in sporting activities and during the growing phase.
Causes
The most common cause of heel pain in adults is plantar fasciitis, which is an inflammation of the band of tissue in the sole that connects the heel to the toes and forms the natural foot arch. Plantar fasciitis may or may not be complicated by a calcaneal spur, a small bone growth that protrudes out of the heel. Plantar fasciitis may also be referred to as plantar fasciosis. In contrast to fasciitis, which essentially means inflammation, fasciosis refers to degeneration of the tissue. In fact, if left untreated, acute plantar fasciitis may develop into a chronic painful condition, which results in slow and irreversible degeneration of the fascia, hence plantar fasciosis. The location of the pain is usually exactly under the heel but may also occur in the arch of the foot. Pain typical to plantar fasciitis is that which feels worse when arising on to your feet such as in mornings or after sitting down for a while, and usually progresses in severity when left untreated.
Symptoms
The symptoms of plantar fasciitis are pain on the bottom of the heel, pain in the arch of the foot, pain that is usually worse upon arising, pain that increases over a period of months. People with plantar fasciitis often describe the pain as worse when they get up in the morning or after they?ve been sitting for long periods of time. After a few minutes of walking the pain decreases, because walking stretches the fascia. For some people the pain subsides but returns after spending long periods of time on their feet.
Diagnosis
The diagnosis of plantar fasciitis is generally made during the history and physical examination. There are several conditions that can cause heel pain, and plantar fasciitis must be distinguished from these conditions. Pain can be referred to the heel and foot from other areas of the body such as the low back, hip, knee, and/or ankle. Special tests to challenge these areas are performed to help confirm the problem is truly coming from the plantar fascia. An X-ray may be ordered to rule out a stress fracture of the heel bone and to see if a bone spur is present that is large enough to cause problems. Other helpful imaging studies include bone scans, MRI, and ultrasound. Ultrasonographic exam may be favored as it is quick, less expensive, and does not expose you to radiation. Laboratory investigation may be necessary in some cases to rule out a systemic illness causing the heel pain, such as rheumatoid arthritis, Reiter's syndrome, or ankylosing spondylitis. These are diseases that affect the entire body but may show up at first as pain in the heel.
Non Surgical Treatment
Clinical trials are underway investigating the use of radiofrequency to treat plantar fasciitis. It is a simple, noninvasive form of treatment. It allows for rapid recovery and pain relief within seven to 10 days. The radio waves promote angiogenesis (formation of new blood vessels) in the area. Once again, increasing blood flow to the damaged tissue encourages a healing response. Antiinflammatory medications are sometimes used to decrease the inflammation in the fascia and reduce your pain. Studies show that just as many people get better with antiinflammatories as those who don't have any improvement. Since these medications are rarely used alone, it's difficult to judge their true effectiveness. A cortisone injection into the area of the fascia may be used but has not been proven effective. Studies show better results when ultrasound is used to improve the accuracy of needle placement. Cortisone should be used sparingly since it may cause rupture of the plantar fascia and fat pad degeneration and atrophy, making the problem worse. Botulinum toxin A otherwise known as BOTOX has been used to treat plantar fasciitis. The chemical is injected into the area and causes paralysis of the muscles. BOTOX has direct analgesic (pain relieving) and antiinflammatory effects. In studies so far, there haven't been any side effects of this treatment.
Surgical Treatment
If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints or a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as open surgery, where the section of the plantar fascia is released by making a cut into your heel or endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team.
how to get rid of heel spurs
Prevention
Being overweight can place excess pressure and strain on your feet, particularly on your heels. Losing weight, and maintaining a healthy weight by combining regular exercise with a healthy, balanced diet, can be beneficial for your feet. Wearing appropriate footwear is also important. Ideally, you should wear shoes with a low to moderate heel that supports and cushions your arches and heels. Avoid wearing shoes with no heels.
Mortons Neuroma Treatment
Overview
 A neuroma is a thickening of nerve tissue that may develop in various parts of the body. The most common neuroma in the foot is a Morton?s neuroma, which occurs between the third and fourth toes. It is sometimes referred to as an intermetatarsal neuroma. ?Intermetatarsal? describes its location in the ball of the foot between the metatarsal bones. Neuromas may also occur in other locations in the foot. MortonThe thickening, or enlargement, of the nerve that defines a neuroma is the result of compression and irritation of the nerve. This compression creates enlargement of the nerve, eventually leading to permanent nerve damage.
A neuroma is a thickening of nerve tissue that may develop in various parts of the body. The most common neuroma in the foot is a Morton?s neuroma, which occurs between the third and fourth toes. It is sometimes referred to as an intermetatarsal neuroma. ?Intermetatarsal? describes its location in the ball of the foot between the metatarsal bones. Neuromas may also occur in other locations in the foot. MortonThe thickening, or enlargement, of the nerve that defines a neuroma is the result of compression and irritation of the nerve. This compression creates enlargement of the nerve, eventually leading to permanent nerve damage.
Causes
In many cases, a neuroma may develop as a result of excessive loading on the front of the foot. Sometimes, a patient?s anatomic alignment in the forefoot contributes to the overload. There may be some cases where the neuroma develops spontaneously, for no obvious reason. However, once the nerve is irritated, pressure from walking, and from the adjacent bony prominences (metatarsal heads), as well as from the intermetatarsal ligament that binds the heads together, all may contribute to persistent pain. Repetitive pressure on the nerve causes localized injury with resulting scarring and fibrosis of the nerve. This leads to symptoms in the distribution of the nerve.
Symptoms
Feelings of numbness, tingling or tenderness in the ball of the foot (the area just behind the base of the toes) are some of the first signs of a condition known as Morton?s Neuroma. However, the condition is somewhat unpredictable, and symptoms may vary from patient to patient. Generally, however, the discomfort gets worse rather than better, and the patient may feel pain or a burning sensation that radiates out to the toes. Eventually, wearing shoes becomes uncomfortable (or even unbearable), and the patient may complain that the feeling is similar to that of having a stone bruise, or walking on a marble or pebble constantly, even though no there is no trauma to the skin, and no visible bump or lump on the sole of the foot.
Diagnosis
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose a Morton's neuroma. Investigations such as an X-ray, ultrasound, MRI, CT scan or bone scan may sometimes be used to assist with diagnosis, assess the severity of the injury and rule out other conditions.
Non Surgical Treatment
You may be able to treat this problem at home. Avoid wearing tight, pointy, or high-heeled shoes. Choose well-fitted shoes with plenty of room for your toes. Put ice or a cold pack on the area for 10 to 15 minutes at a time. Put a thin cloth between the ice and your skin. Take anti-inflammatory medicines to reduce pain and swelling. These include ibuprofen (such as Advil or Motrin) and naproxen (such as Aleve). Rest your feet when you can. Reduce activities that put pressure on the toes, such as racquet sports or running. Try massaging your foot to relax the muscles around the nerve. If these steps do not relieve your symptoms, your doctor may have you use special pads or devices that spread the toes to keep them from squeezing the nerve. In some cases, a doctor may give a steroid shot to reduce swelling and pain. If these treatments do not help, your doctor may suggest surgery.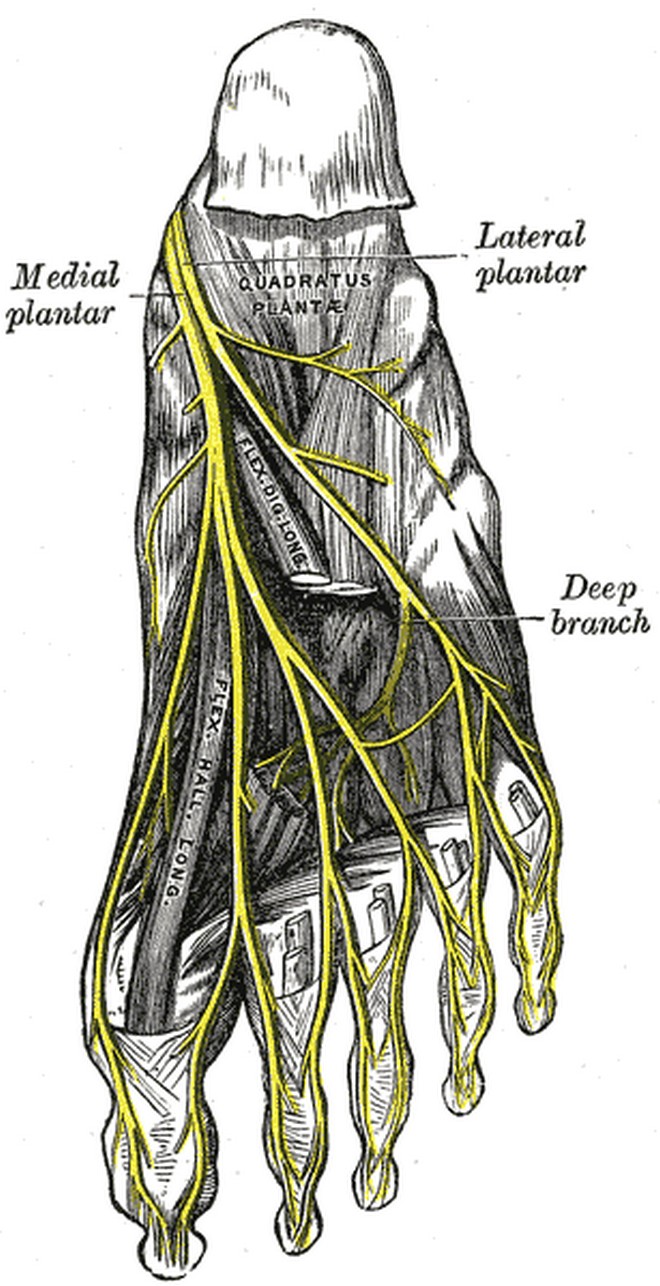
Surgical Treatment
The above measures are often sufficient to resolve Morton?s Neuroma. Should the condition persist or worsen despite these efforts, surgery may be recommended to remove the Neuroma. The surgery requires only a short recovery period, though permanent numbness in the affected toes can result, so such surgery is generally used as a last resort.
Prevention
Wearing shoes that fit properly and that have plenty of room in the toe area may help prevent Morton's neuroma.
A neuroma is a thickening of nerve tissue that may develop in various parts of the body. The most common neuroma in the foot is a Morton?s neuroma, which occurs between the third and fourth toes. It is sometimes referred to as an intermetatarsal neuroma. ?Intermetatarsal? describes its location in the ball of the foot between the metatarsal bones. Neuromas may also occur in other locations in the foot. MortonThe thickening, or enlargement, of the nerve that defines a neuroma is the result of compression and irritation of the nerve. This compression creates enlargement of the nerve, eventually leading to permanent nerve damage.Causes
In many cases, a neuroma may develop as a result of excessive loading on the front of the foot. Sometimes, a patient?s anatomic alignment in the forefoot contributes to the overload. There may be some cases where the neuroma develops spontaneously, for no obvious reason. However, once the nerve is irritated, pressure from walking, and from the adjacent bony prominences (metatarsal heads), as well as from the intermetatarsal ligament that binds the heads together, all may contribute to persistent pain. Repetitive pressure on the nerve causes localized injury with resulting scarring and fibrosis of the nerve. This leads to symptoms in the distribution of the nerve.
Symptoms
Feelings of numbness, tingling or tenderness in the ball of the foot (the area just behind the base of the toes) are some of the first signs of a condition known as Morton?s Neuroma. However, the condition is somewhat unpredictable, and symptoms may vary from patient to patient. Generally, however, the discomfort gets worse rather than better, and the patient may feel pain or a burning sensation that radiates out to the toes. Eventually, wearing shoes becomes uncomfortable (or even unbearable), and the patient may complain that the feeling is similar to that of having a stone bruise, or walking on a marble or pebble constantly, even though no there is no trauma to the skin, and no visible bump or lump on the sole of the foot.
Diagnosis
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose a Morton's neuroma. Investigations such as an X-ray, ultrasound, MRI, CT scan or bone scan may sometimes be used to assist with diagnosis, assess the severity of the injury and rule out other conditions.
Non Surgical Treatment
You may be able to treat this problem at home. Avoid wearing tight, pointy, or high-heeled shoes. Choose well-fitted shoes with plenty of room for your toes. Put ice or a cold pack on the area for 10 to 15 minutes at a time. Put a thin cloth between the ice and your skin. Take anti-inflammatory medicines to reduce pain and swelling. These include ibuprofen (such as Advil or Motrin) and naproxen (such as Aleve). Rest your feet when you can. Reduce activities that put pressure on the toes, such as racquet sports or running. Try massaging your foot to relax the muscles around the nerve. If these steps do not relieve your symptoms, your doctor may have you use special pads or devices that spread the toes to keep them from squeezing the nerve. In some cases, a doctor may give a steroid shot to reduce swelling and pain. If these treatments do not help, your doctor may suggest surgery.
Surgical Treatment
The above measures are often sufficient to resolve Morton?s Neuroma. Should the condition persist or worsen despite these efforts, surgery may be recommended to remove the Neuroma. The surgery requires only a short recovery period, though permanent numbness in the affected toes can result, so such surgery is generally used as a last resort.
Prevention
Wearing shoes that fit properly and that have plenty of room in the toe area may help prevent Morton's neuroma.
Why Shoe Lifts Are The Ideal Solution To Leg Length Imbalances
There are not one but two different kinds of leg length discrepancies, congenital and acquired. Congenital indicates you are born with it. One leg is anatomically shorter than the other. Through developmental phases of aging, the human brain senses the stride pattern and recognizes some variance. Your body usually adapts by tilting one shoulder over to the "short" side. A difference of less than a quarter inch isn't really uncommon, demand Shoe Lifts to compensate and commonly won't have a profound effect over a lifetime.

Leg length inequality goes mainly undiscovered on a daily basis, yet this problem is very easily remedied, and can eliminate a number of incidents of lumbar pain.
Therapy for leg length inequality typically involves Shoe Lifts. Most are affordable, normally being under twenty dollars, compared to a custom orthotic of $200 or higher. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Lower back pain is easily the most prevalent condition afflicting men and women today. Around 80 million people suffer from back pain at some stage in their life. It is a problem that costs businesses millions of dollars annually on account of lost time and productivity. Innovative and improved treatment solutions are always sought after in the hope of minimizing the economical impact this issue causes.

Men and women from all corners of the earth experience foot ache due to leg length discrepancy. In these cases Shoe Lifts are usually of worthwhile. The lifts are capable of alleviating any discomfort in the feet. Shoe Lifts are recommended by many expert orthopaedic practitioners".
So that you can support the body in a balanced manner, feet have a vital task to play. In spite of that, it's often the most overlooked zone of the human body. Some people have flat-feet meaning there is unequal force placed on the feet. This will cause other areas of the body such as knees, ankles and backs to be impacted too. Shoe Lifts make sure that appropriate posture and balance are restored.
Leg length inequality goes mainly undiscovered on a daily basis, yet this problem is very easily remedied, and can eliminate a number of incidents of lumbar pain.
Therapy for leg length inequality typically involves Shoe Lifts. Most are affordable, normally being under twenty dollars, compared to a custom orthotic of $200 or higher. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Lower back pain is easily the most prevalent condition afflicting men and women today. Around 80 million people suffer from back pain at some stage in their life. It is a problem that costs businesses millions of dollars annually on account of lost time and productivity. Innovative and improved treatment solutions are always sought after in the hope of minimizing the economical impact this issue causes.
Men and women from all corners of the earth experience foot ache due to leg length discrepancy. In these cases Shoe Lifts are usually of worthwhile. The lifts are capable of alleviating any discomfort in the feet. Shoe Lifts are recommended by many expert orthopaedic practitioners".
So that you can support the body in a balanced manner, feet have a vital task to play. In spite of that, it's often the most overlooked zone of the human body. Some people have flat-feet meaning there is unequal force placed on the feet. This will cause other areas of the body such as knees, ankles and backs to be impacted too. Shoe Lifts make sure that appropriate posture and balance are restored.
Will A Posterior Calcaneal Spur Cause Pain?

Overview
Heel spurs occur in at least half the people who have plantar fasciitis, a painful condition involving the thick tissue that runs between your heel bone and your toes. In the past, doctors often performed surgery to remove heel spurs, believing them to be the cause of the pain associated with plantar fasciitis. In treating plantar fasciitis now, doctors rely more on ice, arch supports, physical therapy and pain medications, and surgery is rarely performed.
Causes
Heel spurs develop in some people that have a condition called plantar fasciitis, inflammation of the plantar fascia. Heel spurs form when the plantar fascia separates from the calcaneus. An abnormal bone growth, a hook-like spur, forms from calcium deposits that grow at the site of inflammation. Heel spurs are more common in middle-aged adults and people that have had plantar fasciitis for a long time. People with flat feet or high arches are vulnerable to heel spurs. Women who wear high-heeled shoes are more susceptible, as well.

Symptoms
The vast majority of people who have heel spurs feel the asscociated pain during their first steps in the morning. The pain is quite intense and felt either the bottom or front of the heel bone. Typically, the sharp pain diminishes after being up for a while but continues as a dull ache. The pain characteristically returns when first standing up after sitting for long periods.
Diagnosis
Heel spurs and plantar fasciitis is usually diagnosed by your physiotherapist or sports doctor based on your symptoms, history and clinical examination. After confirming your heel spur or plantar fasciitis they will investigate WHY you are likely to be predisposed to heel spurs and develop a treatment plan to decrease your chance of future bouts. X-rays will show calcification or bone within the plantar fascia or at its insertion into the calcaneus. This is known as a calcaneal or heel spur. Ultrasound scans and MRI are used to identify any plantar fasciitis tears, inflammation or calcification. Pathology tests may identify spondyloarthritis, which can cause symptoms similar to plantar fasciitis.
Non Surgical Treatment
Treatment of Heel Spurs is the same as treatment of plantar fasciitis. To arrive at an accurate diagnosis, our foot and ankle Chartered Physiotherapists will obtain your medical history and examine your foot. Throughout this process the physio will rule out all the possible causes for your heel pain other than plantar fasciitis. The following treatment may be used. Orthotics/Insoles. Inflammation reduction. Mobilisation. Taping and Strapping. Rest.
Surgical Treatment
Surgery to correct for heel spur syndrome is a common procedure which releases plantar fascia partially from its attachment to the calcaneous (heel bone). This part of the surgery is called a plantar fasciotomy due to the fact the fascia is cut. This is most often done through an open procedure as any heel spur or bursa can be removed at the same time. If the spur is not removed during the surgery, it will probably be just as successful, as the large spur is not the true problem. Some physicians use an endoscopic approach (EPF) where a small camera aids the physician during surgery with typically smaller incisions on each side of your foot.
Does A Inferior Calcaneal Spur Cause Pain?
Overview
A heel spur is a deposit of calcium on the heel bone. This calcification takes the form of a bony protrusion, which can cause considerable pain when standing and walking. This foot problem is closely related to plantar fasciitis, a condition in which the band of fibrous tissue on the bottom of the foot becomes over-stressed. It pulls away from the heel and causes the calcium deposits to form. For this reason, treating a heel spur involves treating the plantar fascia as well.
Causes
These bony protrusions are commonly found in association with a condition called Plantar Fasciitis. Plantar Fasciitis occurs when the plantar fascia ligament, which spans the arch of the foot, becomes stressed, torn and inflamed. Misalignment and excessive movement of the plantar fascia ligament is most typically the result of an abnormal walking gait. The ligament is designed to stretch with the bounce of each step you take, but if it stretches too much, the resulting small tears and inflammation can cause mild to extreme discomfort. At the same time, it is believed that heel spurs are formed as the body attempts to provide some additional support to the over-stretched ligament. In other words, calcium builds up as a prop to the plantar fascia.

Symptoms
Most of the time heel spurs present as pain in the region surrounding the spur, which typically increases in intensity after prolonged periods of rest. Patients may not be able to bear weight on the afflicted heel comfortably. Running, walking, or lifting heavy weight may exacerbate the issue.
Diagnosis
Most patients who are suffering with heel spurs can see them with an X-ray scan. They are normally hooked and extend into the heel. Some people who have heel spur may not even have noticeable symptoms, although could still be able to see a spur in an X-ray scan.
Non Surgical Treatment
To aid in the reduction of inflammation, applying ice for 10-15 minutes after activities and the use of anti-inflammatory medications, such as aspirin or ibuprofen, can be helpful. Corticosteroid injections may also be used to reduce pain and inflammation. Physical therapy can be beneficial with the use of heat modalities, such as ultrasound, that create a deep heat and reduce inflammation. If the pain caused by inflammation is constant, keeping the foot raised above the heart and/or compressed by wrapping with a bandage will help. Taping can help speed the healing process by protecting the fascia from reinjury, especially during stretching and walking.
Surgical Treatment
In some cases, heel spurs are removed by surgery after an X-ray. While the surgery is typically effective, it?s a timely and expensive procedure. Even after surgery, heel spurs can re-form if the patient continues the lifestyle that led to the problem. These reasons are why most people who develop painful heel spurs begin looking for natural remedies for joint and bone pain. Surgery isn?t required to cure a heel spur. In fact, more than 90 percent of people get better with nonsurgical treatments. If nonsurgical methods fail to treat symptoms of heel spurs after 12 months, surgery may be necessary to alleviate pain and restore mobility.
Prevention
A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don't underestimate your body's need for rest and good nutrition. If obese, lose weight.
What Are Bursitis Of The Foot Indicators
Overview
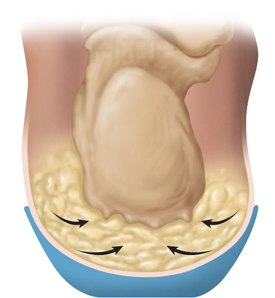
Retrocalcaneal bursitis is sometimes difficult to differentiate from Achilles tendinitis, at least symptomatically. Both are most uncomfortable during the push-off phase of gait, are most severely painful in the morning and with walking after sitting for a period of time, and generally worsen with activity. Most practitioners make the distinction between the two simply on the basis of location of pain and tenderness. Generally, Achilles tendinitis is felt an inch or two higher than this form of bursitis.
Causes
Occasionally the bursal sac can become inflamed and painful. Pain to the region is worse typically with initial weight bearing activity such as rising from bed in the morning. Swelling and warmth to the region are common. Clinical examination shows pain to palpation at the retrocalcaneus at a level just before the Achilles tendon. Increase pressure and friction of the Achilles tendon across the retrocalcaneal region is the cause of this bursitis. A high arch, tight Achilles tendon or bone spur appear to be some of the main causes of this problem. With a high arch the back portion of the calcaneus abnormally projects into the Achilles tendon region.
Symptoms
Pain at the back of the heel at the attachment site of the Achilles tendon when running. Pain on palpation of the back of the heel or bottom of heel. Pain when standing on tiptoes. Swelling and redness at the back and bottom of the heel.
Diagnosis
When a patient has pain in a joint, a careful physical examination is needed to determine what type of movement is affected and if there is any swelling present. Bursitis will not show up on x-rays, although sometimes there are also calcium deposits in the joint that can be seen. Inserting a thin needle into the affected bursa and removing (aspirating) some of the synovial fluid for examination can confirm the diagnosis. In most cases, the fluid will not be clear. It can be tested for the presence of microorganisms, which would indicate an infection, and crystals, which could indicate gout. In instances where the diagnosis is difficult, a local anesthetic (a drug that numbs the area) is injected into the painful spot. If the discomfort stops temporarily, then bursitis is probably the correct diagnosis.
Non Surgical Treatment
Caregivers may give you special shoe inserts with a cutout around the tender area. You may also be told to wear shoes with a reinforced heel counter. This will give better heel control. You may need other shoe inserts (wedges) to raise your heel so it does not press against the back of the shoe. You may also wear shoes that are open in the back, such as sandals that have no strap across the heel. You may use ibuprofen (eye-bu-PROH-fen) and acetaminophen (a-seet-a-MIN-oh-fen) medicine for your pain. These may be bought over-the-counter at drug or grocery stores. Do not take ibuprofen if you are allergic to aspirin. You may be given shots of medicine called steroids (STER-oids) to decrease inflammation. Caregivers may add local anesthesia (an-es-THEE-zah) to the steroids. This medicine helps decrease bursitis pain. Because these shots decrease swelling and pain, you may feel like your ankle is healed and that you can return to heavy exercise. It is important to not exercise until your caregiver says it is OK. You could make the bursitis worse if you exercise too soon. You may need surgery to remove the bursa or part of your ankle bone. Surgery is usually not necessary unless the bursitis is very bad and does not heal with other treatments. Your caregiver may want you to go to physical (FIZ-i-kal) therapy (THER-ah-pee). Physical therapists may use ultrasound to increase blood flow to the injured area. Caregivers may use massage to stretch the tissue and bring heat to the injury to increase blood flow. These and other treatments may help the bursitis heal faster. Exercises to stretch your Achilles tendon and make it stronger will be started after the bursitis has healed. You may gradually increase the amount of weight you put on your foot when caregivers say it is OK. You may be told to stop exercising if you feel any pain.
Surgical Treatment
Surgery is rarely done strictly for treatment of a bursitis. If any underlying cause is the reason, this may be addressed surgically. During surgery for other conditions, a bursa may be seen and removed surgically.
Retrocalcaneal bursitis is sometimes difficult to differentiate from Achilles tendinitis, at least symptomatically. Both are most uncomfortable during the push-off phase of gait, are most severely painful in the morning and with walking after sitting for a period of time, and generally worsen with activity. Most practitioners make the distinction between the two simply on the basis of location of pain and tenderness. Generally, Achilles tendinitis is felt an inch or two higher than this form of bursitis.
Causes
Occasionally the bursal sac can become inflamed and painful. Pain to the region is worse typically with initial weight bearing activity such as rising from bed in the morning. Swelling and warmth to the region are common. Clinical examination shows pain to palpation at the retrocalcaneus at a level just before the Achilles tendon. Increase pressure and friction of the Achilles tendon across the retrocalcaneal region is the cause of this bursitis. A high arch, tight Achilles tendon or bone spur appear to be some of the main causes of this problem. With a high arch the back portion of the calcaneus abnormally projects into the Achilles tendon region.
Symptoms
Pain at the back of the heel at the attachment site of the Achilles tendon when running. Pain on palpation of the back of the heel or bottom of heel. Pain when standing on tiptoes. Swelling and redness at the back and bottom of the heel.
Diagnosis
When a patient has pain in a joint, a careful physical examination is needed to determine what type of movement is affected and if there is any swelling present. Bursitis will not show up on x-rays, although sometimes there are also calcium deposits in the joint that can be seen. Inserting a thin needle into the affected bursa and removing (aspirating) some of the synovial fluid for examination can confirm the diagnosis. In most cases, the fluid will not be clear. It can be tested for the presence of microorganisms, which would indicate an infection, and crystals, which could indicate gout. In instances where the diagnosis is difficult, a local anesthetic (a drug that numbs the area) is injected into the painful spot. If the discomfort stops temporarily, then bursitis is probably the correct diagnosis.
Non Surgical Treatment
Caregivers may give you special shoe inserts with a cutout around the tender area. You may also be told to wear shoes with a reinforced heel counter. This will give better heel control. You may need other shoe inserts (wedges) to raise your heel so it does not press against the back of the shoe. You may also wear shoes that are open in the back, such as sandals that have no strap across the heel. You may use ibuprofen (eye-bu-PROH-fen) and acetaminophen (a-seet-a-MIN-oh-fen) medicine for your pain. These may be bought over-the-counter at drug or grocery stores. Do not take ibuprofen if you are allergic to aspirin. You may be given shots of medicine called steroids (STER-oids) to decrease inflammation. Caregivers may add local anesthesia (an-es-THEE-zah) to the steroids. This medicine helps decrease bursitis pain. Because these shots decrease swelling and pain, you may feel like your ankle is healed and that you can return to heavy exercise. It is important to not exercise until your caregiver says it is OK. You could make the bursitis worse if you exercise too soon. You may need surgery to remove the bursa or part of your ankle bone. Surgery is usually not necessary unless the bursitis is very bad and does not heal with other treatments. Your caregiver may want you to go to physical (FIZ-i-kal) therapy (THER-ah-pee). Physical therapists may use ultrasound to increase blood flow to the injured area. Caregivers may use massage to stretch the tissue and bring heat to the injury to increase blood flow. These and other treatments may help the bursitis heal faster. Exercises to stretch your Achilles tendon and make it stronger will be started after the bursitis has healed. You may gradually increase the amount of weight you put on your foot when caregivers say it is OK. You may be told to stop exercising if you feel any pain.
Surgical Treatment
Surgery is rarely done strictly for treatment of a bursitis. If any underlying cause is the reason, this may be addressed surgically. During surgery for other conditions, a bursa may be seen and removed surgically.